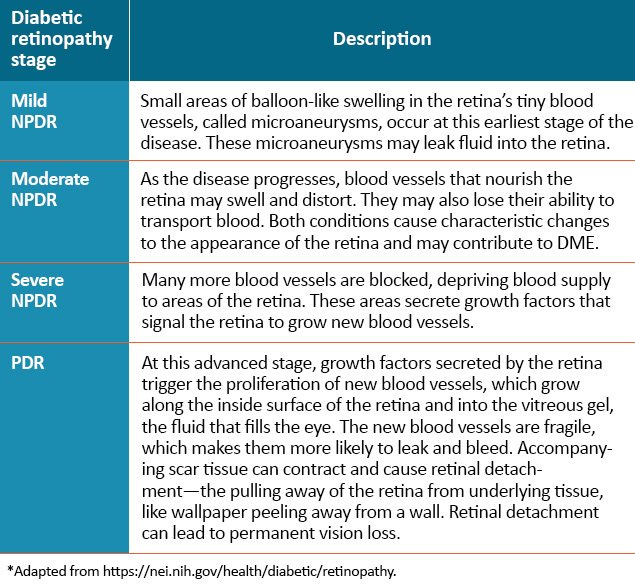
DME = diabetic macular edema; NPDR = nonproliferative diabetic retinopathy; PDR = proliferative diabetic retinopathy.
Chronic hyperglycemia induces oxidative stress through a variety of potential pathways, resulting in alterations of metabolic homeostasis within the retina. These changes can initiate compensatory responses, instigating vascular dilation and increased retinal blood flow.3-5
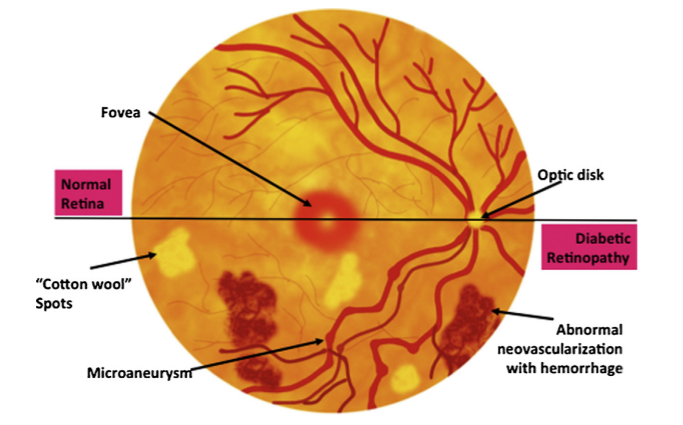
Pericytes — cells within retinal capillary walls that provide physical strength and biochemical support to underlying endothelial cells — are damaged and ultimately lost. Consequently, the integrity of endothelial cells can be compromised, leading to the development of localized outpouchings in capillary walls, called microaneurysms. This is the earliest clinically evident stage of diabetic retinopathy. Subsequently, the integrity of the outer blood-retina barrier is impaired, eventually resulting in the leakage of plasma into the surrounding neural tissues.3-5
Chronic hyperglycemia and oxidative stress also stimulate an inflammatory response within many cell types, including vascular endothelial cells. Increased leukocyte-endothelium adhesion may cause endothelial and neuroglial cell injury by capillary occlusion. Injury may also occur through the release of inflammatory mediators triggered by tissue hypoxia.1,3-8
Retinal hypoxia and ischemia — as well as microglial hyperglycemia — lead to the upregulation and secretion of multiple cytokines, including vascular endothelial growth factor (VEGF). Diffusible VEGF has three complementary roles, including driving endothelial cell proliferation — or angiogenesis — increasing vascular permeability, and increasing local inflammatory infiltrates.1,6-8
VEGF can promote endothelial expression of intercellular adhesion molecule-1 (ICAM-1), inciting leukocyte activation and cytokine release, which leads to additional cytokine secretion — including VEGF — with continued propagation of the inflammatory response. Chronic inflammation contributes to capillary occlusion and breakdown of the blood-retinal barriers critical for normal retinal homeostasis under physiologic conditions.1,6-8
Long-term, increased plasma leakage and continued pericyte loss can cause further breakdown of the inner blood-retina barrier, with ensuing vascular degenerative changes, such as endothelial cell apoptosis and basement-membrane thickening. Vascular swelling and structural distortion stemming from the loss of integrity in the blood-retina barrier eventually result in capillary occlusion and ischemia, increasing plasma leakage and progression of the continuum of diabetic macular edema (DME).1-8
The pathogenesis of DME is at this time poorly defined, but is believed to involve angiogenesis, inflammation, and oxidative stress.9,10 The pathophysiology of DME involves dilated capillaries, retinal microaneurysms, and loss of pericytes, with eventual impairment of the blood-retinal barrier (BRB).11,12 Breakdown of the BRB results in fluid leakage into the extracellular space, which disrupts macular structure and function on a cellular level.13 Hyperglycemia is reported to lead to capillary endothelial damage and alterations in leukocyte function;14 additionally, hyperglycemia has been reported to activate oxidative stress agents, such as advanced glycation end products and the protein kinase C (PKC) pathway.11,15 Various inflammatory mediators appear to play a role in promoting DME, including VEGF, placental growth factor (PlGF), hepatocyte growth factor (HGF) and others.10,11,16-18